
This is post #2 in the #RootCauseRacism series...
As we explore concepts like psychological safety and Diversity, Equity, Inclusion, and Accessibility (DEIA) in this blog post series, I’d like to kick things off with a look at some serious problem statements that we must address. I’m thankful for the organizations, including Value Capture clients, who aim to close these performance gaps in systematic and sustained ways.
In 2023, healthcare organizations face a number of serious problems. For one, patients continue to be harmed at unacceptably high rates, not because of “bad providers,” but as the result of preventable errors that are caused by process problems and miscommunications.
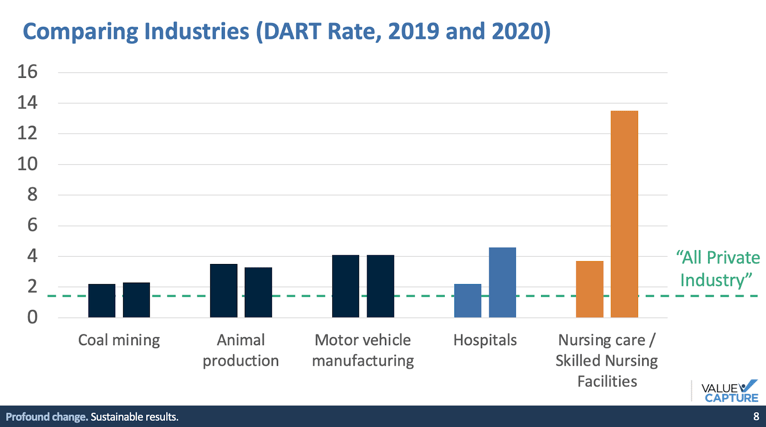
Additionally, healthcare professionals are injured at rates far higher than in industries that are perceived as dangerous, such as mining or manufacturing, as the chart below (driven by OSHA data) shows:
For measures such as various types of patient harms (including pressure ulcers, falls, and hospital-acquired infections) — and employee injuries and lost workdays — we need to define the measurable gaps between current levels of performance and the theoretical limits — zero harm. It’s not just the averages that matter, but the variation. Nobody should get hurt at work, but how can we identify inequities in health outcomes and employee safety data, with the aim of providing equally safe conditions for all?
If organizations and their senior leaders cannot openly admit serious problems, like patient or employee harm, how can they expect healthcare professionals to speak up about the problems and causes of harm that they see and experience?
If people are going to choose to use their voice, we need to eliminate the two primary barriers, as discussed by Ethan Burris, Ph.D. from the University of Texas at Austin: fear and futility. If people fear punishment, they won’t speak up. Even if the fear factor is reduced, people will stop speaking up if they think doing so isn’t worth the effort.
Others will discuss this concept, and its practical implications, so let’s start with a definition of “psychological safety” to get us on the same page. Timothy R. Clark, Ph.D., author of The 4 Stages of Psychological Safety, defines it as:
“Psychological safety is a social condition in which you feel:
- Included
- Safe to learn
- Safe to contribute
- Safe to challenge the status quo
… all without fear of being embarrassed, marginalized, or punished in some way.”
You can take a deeper dive into psychological safety through this Value Capture resources page.
Research by Amy Edmondson, Ph.D., from Harvard Business School, has demonstrated that teams with the highest levels of psychological safety improve more and perform better — whether that’s within a tech company like Google or a healthcare organization.
In healthcare teams, having a higher feeling of psychological safety means individuals are more likely to speak up about risks, problems, mistakes, near-misses, or harm. We cannot solve problems unless we know what they are. Speaking up about a near-miss means that future harm can be prevented.
When leaders can reduce fear, people will feel safer about speaking up. That’s the fear factor. That must be followed up with effective problem-solving, speaking up about a mistake means that it won’t be repeated. We reduce the futility factor, as well.
How do leaders create conditions for people to feel psychologically safe? They cannot declare an organization, or some part of it, to be a “safe space;” they must demonstrate that it’s actually safe to speak up without the fear of (or the reality of) punishment. It’s neither fair nor effective to demand that healthcare professionals be brave or courageous, or that it’s their professional obligation to speak truth to power.
When fear exists, people will protect themselves by choosing to stay silent. That’s their right and it’s understandable. That’s why leaders must work to reduce the level of risk — shifting from punishing those who speak up to instead rewarding and celebrating them for doing so. As Clark teaches, leaders set the tone through not just their words, but their actions. Those actions include two high-level countermeasures:
- Modeling vulnerable acts
- Rewarding vulnerable acts
As Clark says, a “vulnerable act” is one that exposes us to the risk of harm or loss, personally or professionally. Writing a blog post like this is a vulnerable act in the sense that an author might say the wrong thing that offends, or they might hurt their professional reputation by writing something that’s unclear. Any human interaction is, on some level, a vulnerable act. If we don’t feel a low level of risk (or zero risk), then our leaders and colleagues can work to help us feel safer over time.
Other examples of vulnerable acts, mapped to Clark’s 4 Stages model can be found below:
|
Stage |
Name |
Example of a Vulnerable Act |
|
1 |
Inclusion Safety |
Sharing a personal problem or challenge |
|
2 |
Learner Safety |
Sharing past mistakes |
|
3 |
Contributor Safety |
Communicating bad news |
|
4 |
Challenger Safety |
Inviting others to challenge your opinion |
Because of their leadership position, these acts are generally less vulnerable (or less risky) to a more senior leader. Leading by example gives others permission to follow. Some acts, such as actively inviting disagreement, debate, or dissent, directly give people permission to use their voices. But people might still be afraid, especially if speaking up was punished by previous leaders.
Telling people they should now feel safe doesn’t mean they will immediately feel safe. If a leader has admitted a mistake or disclosed that they don’t know something, team members might test the waters in a small way that doesn’t feel horribly unsafe. When employees mirror those vulnerable acts or respond to the invitation to speak up, leaders must reward them for doing so.
In Clark’s model, teams and organizations generally progress through the four stages of psychological safety. The ultimate level, the most difficult for a team to achieve, would be Stage 4 “challenger safety” where people feel safe challenging the status quo. This is where improvement and innovation happen. But it’s hard for people to feel safe challenging the status quo if they don’t first feel included, accepted, and respected by their colleagues and leaders.
Stage 1 “inclusion safety” is closely connected to Diversity, Equity, Inclusion, Accessibility (DEIA) and Belonging goals, practices, and initiatives. If all employees don’t feel equal levels of inclusion safety, due to gender, race, ethnicity, sexual orientation, or other distinguishing characteristics, then we can’t expect them to feel equally safe to learn, contribute, and challenge the status quo.
If employees from different demographic groups don’t feel equally included, they would feel less welcome to ask questions, and less safe to challenge the status quo. This means that staff safety and patient safety, in their departments, will suffer. As this article says, “The main stressor many Black women face is a lack of psychological safety,”
As this Forbes article says:
“Frustratingly, Black women also ranked dead last in their experience of manager support—managers showing interest in their career, checking in on their well-being and promoting inclusion—as compared [to survey results grouped by] other identities including men, all women, LGBTQ women, women with disabilities, white women, Asian women, and Latinas.”
In a healthcare organization, if leaders are committed to equity in employee safety and in health outcomes, I suggest asking the following questions:
- Are there disparities in patient safety measures or other health outcomes based on demographics?
- Are there disparities in employee safety metrics, including lost workday incidents, based on demographics?
- Are employee safety disparities caused, to what degree, by the type of work being more physically demanding, or caused by some employee groups feeling less safe to speak up?
- What can we do to reduce gaps in the feeling of psychological safety across teams or demographic groups?
- What hypotheses can we test and how would we gauge our progress?
As we kick off this blog series, I look forward to the contributions from our varied and diverse contributors. I am also eager to hear thoughts, comments, questions, and experiences from our audience, here and on social media.
Thanks for reading! Thanks to Value Capture for sponsoring this series. Thanks to Deondra Wardelle for her guidance and collaboration. And thanks to everybody who has contributed.


Written by Mark Graban
Mark Graban has served healthcare clients since 2005. Mark is internationally recognized as a leading author and speaker on Lean healthcare. His latest book is "The Mistakes That Make Us: Cultivating a Culture of Learning and Innovation."
Submit a comment